Introduction and objective
Although MRI targeted biopsies (TBx) have been demonstrated to provide high accuracy in detecting clinically signicant prostate cancer (PCa), the addition of systematic biopses (SBx) is still necessary since up to 10% of clinically signicant prostate cancer (csPCa) may be missed by TBx. However, little is known about the interaction between the morphological features of the index lesion (IL) and the added value of SBx. We hypothesized that the need for SBx for the detection of csPCa may vary signicantly according to the features of the IL.
Methods
We relied on 1,922 men who underwent MRI of the prostate with subsequent fusion TBx and concomitant SBx at three referral centres between 2013 and 2020. For this study purposes, we identied 1,345 men with single MRI suspicious, dened as the IL. Only men with positive MRI dened as any lesion with PI-RADS ≥3 were included. The study outcome was the added value of SBx in the detection of csPCa (dened any Gleason grade ≥2 detected at SBx and missed by TBx). Thereafter, we explored the correlation between the added value of SBx and the IL volume using Lowess function. All analyses were adjusted for age, PSA, prostate volume, PI-RADS and number of targeted cores of the IL.
Results
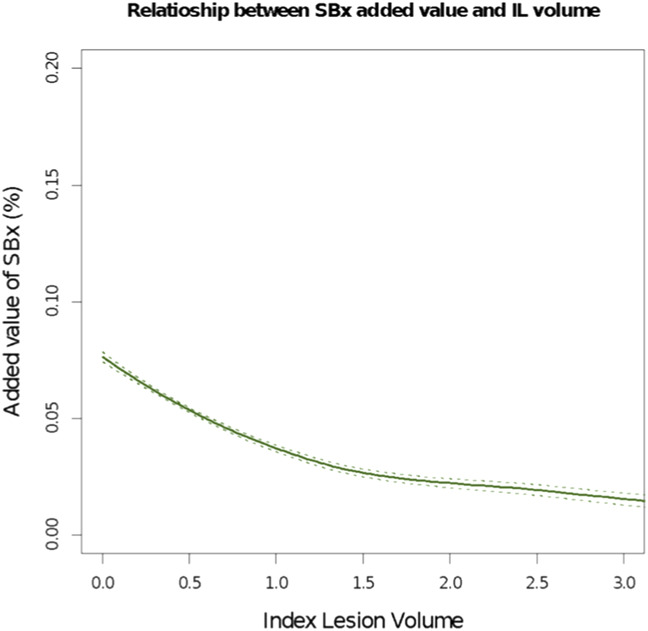
Overall, 569 (42%) men had csPCa at TBx of all lesions. On the contrary, 419 (31%) men had csPCa at SBx. The median added value of SBx was 6%, corresponding to 74 csPCa missed by TBx and identied by SBx. The median volume of IL was 0.6 cc (IQR: 0.3-1.5cc). At MVA, higher PI-RADS score of the IL and number of cores targeting the IL did not independently impact the added value of SBx for the detection of csPCa (all p>0.2). On the other hand, increasing IL volume was associated with lower probability of detecting csPCa at SBx that may be missed at TBx (OR 0.59, p=0.038). At Lowess, the added value of SBx dropped from 8 to 3% between IL volume of 0.1 and 1.5cc (p=0.01). A plateau could be identied for IL larger than 1.5 cc (Figure 1).
Conclusions
We demonstrated that an IL with an estimated volume larger than 1.5 cc can be biopsied by TBx only since the added value of SBx for the detection of csPCa is very limited. By using this approach, approximately 25% of men would receive a TBx only without compromising the risk of underestimating the burden of csPCa.
Figure 1