Research Funding
Pfizer Inc. and Astellas Pharma, Inc
Background
The PROSPER trial demonstrated prolonged MFS and OS for men with nmCRPC and rapidly rising PSA treated with ENZA vs placebo, both in combination with androgen deprivation therapy (ADT). The final survival analysis of PROSPER (Sternberg et al. NEJM 2020) recently reported a median OS of 67.0 months (95% CI, 64.0 to not reached) with ENZA and 56.3 months (95% CI, 54.4 to 63.0) with placebo (hazard ratio [HR] for death, 0.73; 95% CI, 0.61 to 0.89; P = .001). Post hoc analyses of PROSPER evaluating PSA dynamics have demonstrated longer MFS with greater PSA decline (Hussain et al. ESMO Sept 19-21, 2020. Poster 685P) and increased risk of metastases in patients with even modest PSA progression vs those without (Saad et al. Eur Urol 2020). Here we further explored the relationship between PSA dynamics and outcomes in PROSPER using uniquely defined PSA subgroups of decline.
Methods
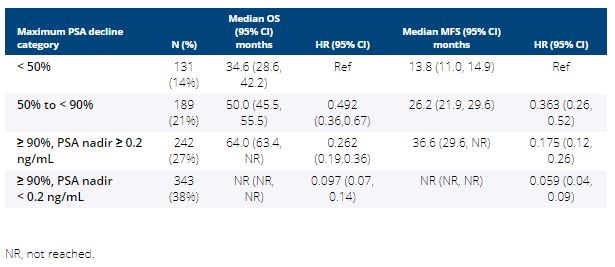
Eligible men in PROSPER had nmCRPC, a PSA level ≥ 2 ng/mL at baseline, and a PSA doubling time ≤ 10 months. Men continued ADT, were randomized 2:1 to ENZA 160 mg once daily vs placebo, and had PSA evaluation at week 17 and every 16 weeks thereafter. This post hoc analysis evaluated OS and MFS for 4 mutually exclusive subgroups defined by PSA nadir using men with PSA reduction < 50% as the reference group. The HR is based on an unstratified Cox proportional hazards analysis model.Results:1401 men were enrolled in PROSPER; 933 were treated with ENZA and PSA data were available for 905. Measured at nadir, 38% of these men achieved PSA reduction ≥ 90% (actual nadir < 0.2 ng/mL), and another 27% achieved PSA reduction ≥ 90% (actual nadir ≥ 0.2 ng/mL). Among men in the placebo arm of PROSPER only 3/457 reported PSA reduction ≥ 90%. Median OS and MFS increased with increasing depth of PSA decline (Table).
Conclusions
In men with nmCRPC and rapidly rising PSA treated with ADT plus ENZA, there was a close relationship between the degree of PSA decline and survival outcomes. Defining PSA by both percent decline and actual decline below 0.2 ng/mL revealed a previously under-appreciated relationship between these PSA metrics and highlights the importance of PSA nadir as an intermediate biomarker in nmCRPC. Clinical trial information: NCT02003924